Since the publication of its new strategy and in the ongoing conversations with providers, CQC has signalled a clear and welcome shift in its approach. It has committed to a leaner, more proportionate and risk-based approach, with a stronger focus on safety, leadership, and a smart use of data and intelligence. The intention is to create a system of regulation which is more flexible, relevant and fit for purpose, aligned to system working, able to measure quality of care across pathways and help tackle health inequalities.
Views on CQC’s new regulatory approach
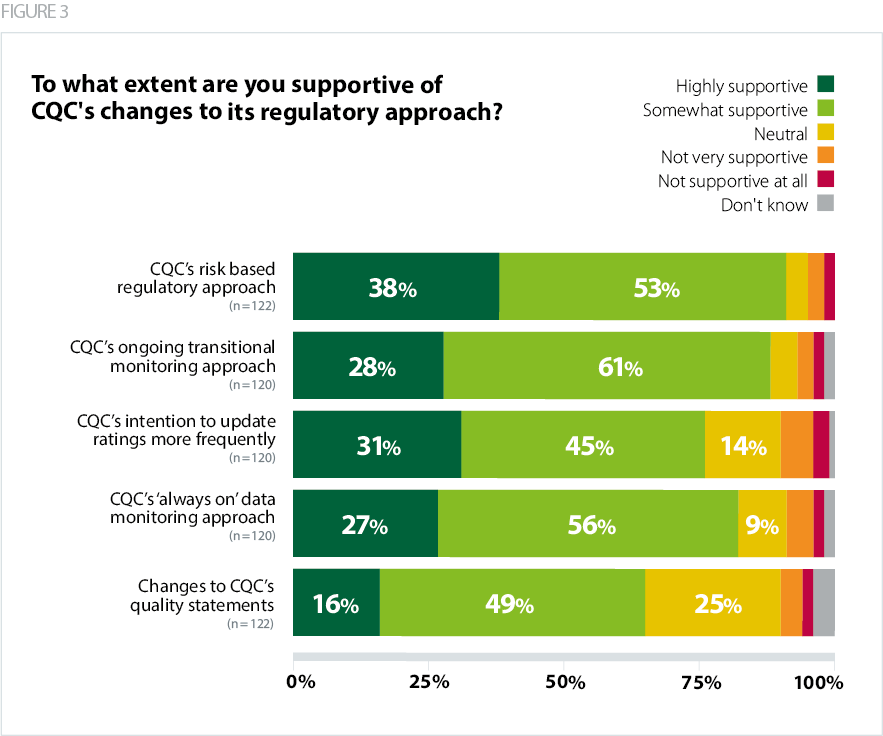
As a result of the pandemic, providers are already working more collaboratively as part of systems, and they appreciate the new approach CQC has committed to. Our survey shows overwhelming support for CQC’s new risk-based approach – 91% of respondents were highly supportive or somewhat supportive.
A similarly high percentage (89%) were supportive of CQC’s ongoing transitional monitoring approach, which aims to prioritise its activity with a focus on safety. More than four in five trust leaders (83%) supported CQC’s ‘always on’ data monitoring approach, which has moved away from scheduled inspections and aims to be more flexible and responsive to changes in quality and safety within services.
There were high levels of support for CQC’s updated inspection methodology. Just over three quarters of respondents (76%) supported CQC’s intention to update ratings more frequently, in order to provide an up-to-date picture of quality. Nearly two thirds (65%) were supportive of changes to CQC’s quality statements, which are now being framed as 'We' statements.
Trust leaders agreed with changes to CQC’s approach, but were waiting for these to be realised in implementation – for example ensuring the new approach is equally applicable to all sectors:
A positive step but must be reflective of the different sectors and not fall into the trap of retrofitting everything around hospital services and operating models.
Respondents highlighted the importance of the quality of data and its interpretation. Some pointed out that the data CQC uses is outdated, and others commented that some sectors have limited or low data sources (for example the community and mental health sectors), which may be a barrier.
Trusts also recognise that CQC's new regulatory approach would only work if it accounts for system working, and the complexity and interrelatedness of many of the issues the sector is currently facing:
There is increasing recognition that trusts are not 'islands' but operate within a highly complex system. Yet the solutions to problems, seen at the time of inspection, are often to be found in shared/joint solutions. There should be greater recognition of this so that recommendations are framed within the areas that the Trust has influence over and the areas where responsibilities are shared or lie outside of the Trust's direct control.
Experiences of CQC regulation
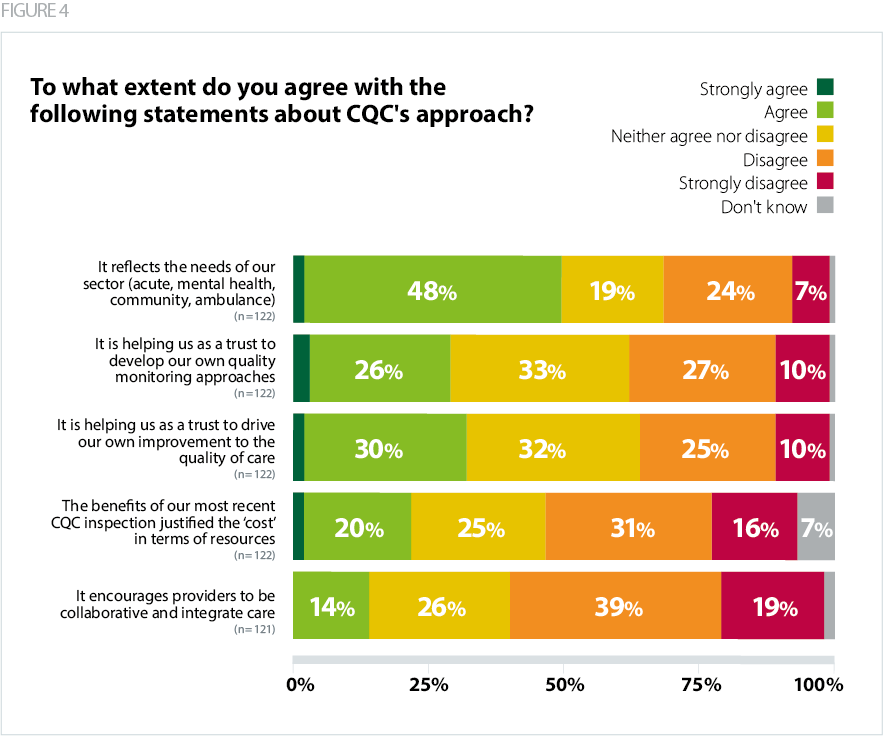
In contrast to the overwhelming support for CQC’s new modern and flexible approach, providers were less positive about their current experiences of the CQC.
- Half of respondents (50%) agreed that CQC’s approach reflects the needs of their sector, and 31% disagreed.
- Just under a third of respondents agreed that CQC’s approach is helping them develop their own quality monitoring approaches, and their own improvement in the quality of care.
- Almost a third agree (32%) that CQC’s approach is helping them as a trust to drive their own improvement in the quality of care.
- An even smaller proportion of respondents (22%) agreed that the benefits of their most recent CQC inspection justified the ‘cost’ in terms of resources spent to prepare and host the inspection team.
- Only 14% agreed that CQC's approach to regulation encourages providers to be collaborative and integrate care, while 58% disagreed.
Comments showed that trust leaders feel that CQC, despite its evolving strategic approach, is still predominantly focused on individual organisations, rather than pathways or systems. More clarity was needed on its approach to regulating systems, places and provider collaboratives.
The responsibility and accountability of individual trusts to meet CQC requirements and inspection of individual trusts does not encourage collaboration or look to address root causes that may exist outside individual organisations.
There was also a perception that, by focusing on individual organisations, CQC was still unable to identify system problems and encourage system solutions:
Whilst the regulatory framework is helpful for Trusts I do not currently feel that the CQC approach reflects the issues and pressures that exist within our system, and the impact of these on our Trust performance.
CQC inspection activity
In our survey we asked trusts about the types of CQC inspection they had undergone in the past 12 months. We found that the majority of respondents (61%) had undergone a focused inspection, in contrast with just under a third of respondents, who had undergone a core service with well-led inspection. A very small number – just 8% of trusts – reported experience of a comprehensive inspection in the past 12 months. This trend is consistent with CQC’s decision to scale back its inspection activity in response to the COVID-19 pandemic, and gradually resuming it in 2021.
We probed trusts’ experience of a well-led inspection with an open-ended question asking how helpful it had been for their organisation. Some respondents highlighted the administrative burden required and the difficulty in sourcing appropriate settings for interviews under the infection prevention and control guidelines at the time.
However, others found that well-led inspections were helpful in confirming what they already knew, and in some cases led to a beneficial outcome such as a re-rating, or a recommendation to remove the trust from the recovery support programme. Some mentioned that the interviews were thorough and that the inspections were fair and proportionate.
The team was smaller than we had previously experienced and inspectors were suitably experienced. The report was a fair representation of us as an organisation. A significant amount of preparatory work was required by a large number of individuals in advance and it was a logistical challenge to manage rooms (in the midst of Covid restrictions) for interviews in person.
CQC's new powers to review and assess ICSs and local authorities
We asked trust leaders about their opinion on the important factors for CQC to consider as it develops its approach to assessing the performance of systems, including its new single assessment framework for ICSs, local authorities and providers.
We received a large number of responses to this question. The main emerging themes were:
- clarifying where responsibilities and accountability lie, in terms of statutory and regulatory
- responsibilities and making sure risks in the system are managed
- clarifying the approach to regulating provider collaboratives
- building on existing work to offer more consideration clarifying the approach to regulating providers within provider collaboratives
- assessing collaborative working across a whole system, including at an ICS and place level, and appropriate involvement of local authorities and the wider health and care sector
- identifying the difference between 'commissioning gaps' and gaps in provision, including appropriate consideration of social care capacity
- focusing on outcomes for patients and the population, including a clear focus on health inequalities
- making sure the voice of users and staff is taken into account and acted upon
- focus on a culture of improvement in systems
- consideration of financial and workforce challenges within systems
- assessing providers which span multiple ICSs (such as ambulance trusts).
How practically the entire system is assessed, including how the regional providers who span multiple ICSs are taken into account, without undue burden relating to multiple ICS inspections.
Some respondents also mentioned the importance of having a CQC team that understands system working and integrated care, ideally having experience of working in systems.
That assessments consider the whole pathway approach. That CQC teams reflect better the integrated system approach with a mixed skill set and experience amongst inspectors. Ideally inspectors need to have experience working in a system way themselves.
Respondents also highlighted that the whole system is currently undergoing change and CQC needs to be mindful of that, accounting for both the different levels of development between ICSs and the tensions within systems.
Proportionality is always key and inevitably we will be undergoing changes to the system and also the organisations within it. This will be alongside many other drivers for both the system and the providers. CQC need to balance all of these activities and be part of the solution rather than the problem.