
Working better together in neighbourhoods
What is happening now?
Neighbourhood working is not new.
We live, work and play in neighbourhoods and much of our daily experience is shaped by them. It is not surprising that focusing on how we work together better at this level, has been the foundation of many effective and innovative responses to local needs across health and care and beyond.
Neighbourhoods and community-led responses took on particular prominence during the COVID-19 pandemic, but effective interventions at this level pre-dated this experience and continue in a diversity of forms today. The government’s shift to a neighbourhood health service is a cornerstone of its new health policy but also builds on earlier work within the NHS to try to develop better co-ordinated, more local approaches to health and care delivery, including the concept of INTs.
Our evidence suggests that meaningful involvement from across a range of different groups and organisations is key to developing a deep and shared understanding of local health issues and inequalities and an impactful response to these. Achieving this in practice is complicated and requires navigating a range of issues, from how neighbourhoods are defined, to how resources are allocated and how decisions are made.
We have found that the there is no single definition of a neighbourhood across the case studies included in our research.
Local people define their neighbourhoods in ways that reflect the geography, history and culture of where they live, as well as political and socio-economic factors.
Statutory services define neighbourhoods using boundaries such as the shared footprints of GP practices constituting a primary care network, or the wards of a district council, which often only coincidentally represent the neighbourhood that residents identify with. And as a result, population sizes vary greatly from potentially a single row of residencies with up to 50,000 people or more.
In urban areas a neighbourhood may cover a small geographical area, whereas in rural areas, where the population is dispersed, the geographical footprint may in some cases be much larger.
From our case studies, literature review and wider work on community development, it is apparent that enabling a degree of self-determination of neighbourhoods is important to supporting authentic community engagement. But, the case studies also suggest that it is possible for statutory-defined neighbourhood work to still achieve positive outcomes.
In some examples, NHS and local authority partnerships often constructed at a place level have combined statutory-defined boundaries with a flexibility on how smaller-scale neighbourhood work happens and is supported within these boundaries. What is important in all these cases is not necessarily spending significant time and resources on definitions, but rather to acknowledge and manage the potential tension between how systems might define neighbourhoods and how communities and people define their neighbourhoods early on.
Where this tension has been successfully resolved, it has required an openness from statutory partners to work in ways that are as flexible and influenced by community preferences as possible, alongside a recognition from non-statutory partners that this may need to be balanced against what is possible and pragmatic from a statutory perspective.
Working at a neighbourhood level is key to understanding and responding to specific population health issues and inequalities, but it can be complicated by the need to encompass a diversity of local communities with different characteristics, expectations and needs. Some examples of successful neighbourhood working we observed were established specifically to bring a set of local communities together, rather than to continue to work with a disaggregated group of different faith, cultural or interest-based groups.
Neighbourhood working as described in this report can be conceptualised in the middle of a spectrum that ranges from wholly community led to wholly statutory led. This is not to say that other models and interventions are not good examples of neighbourhood working, but many of the strongest examples of sustainable and impactful work sit somewhere in the middle of this spectrum. This is particularly true in more deprived areas, where without statutory support the assets and infrastructure to enable communities to support and enhance their own health and wellbeing may simply not exist, irrespective of the commitment and energy of the local population.
In the aftermath of the Fuller stocktake, endorsed by the chief executives of NHS England and all 42 ICSs, there has been a particular focus on integration at the neighbourhood level within the NHS. This is expressed in the idea of an integrated neighbourhood team (INT) covering health and care professionals working together with voluntary, community and social enterprise (VCSE) organisations and other partners to improve population health outcomes.
Integration in this context is often driven by a desire to provide a more joined-up, efficient and effective approach to prevention, access and complex care.
However, our work suggests that when it comes to working with communities and community groups themselves, positive outcomes can often be achieved simply through better understanding, collaboration and connectivity, without formal integration of teams, funding and approaches. This may also provide lessons for statutory partners looking to enhance joint working on a local and hyper-local scale.
In practice, neighbourhood working generally involves a range of different activities that in some cases are about formal integration and in others are more about cooperation and coordination. This more nuanced approach is a source of strength in many examples. Tools such as the spectrum of collaboration can help to support situating arrangements in terms of local objectives and needs, and what the best response to these is likely to be.
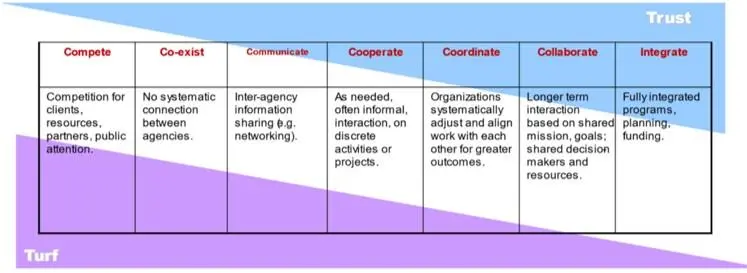
Source: Collaboration Spectrum Revisited (tamarackcommunity.ca)
It is possible to have integrated outcomes, shared between partners, without integrated delivery of the steps to achieve those outcomes. None of our case studies for this report exhibited full integration of statutory and non-statutory services, and we heard in some examples how full integration would likely have led to the models being less effective. We also heard of models where non-statutory services have been able to reach communities and build trust with neighbourhoods in part because they are not seen as being ‘from’ statutory services. Integrating such services more formally with statutory partners would risk breaking this trusting relationship and severing connections with the communities they serve, making future relationships harder to build. This applies particularly to communities where people feel poorly served by statutory services in the past, and therefore currently have a high-level of distrust of these services.
The level of integration in and across any model will need to be defined and guided by the outcomes being sought and needs to be considered carefully as a means to an end, and not an end in itself.