
Working better together in neighbourhoods
Appendices
Methodologies for community working
Public Health England’s review of community-centred approaches identified a family of different approaches underpinned by a range of methodologies. A mix of these is found in many of the examples we have examined. There is no one correct approach and methods need to be adapted to the local context.
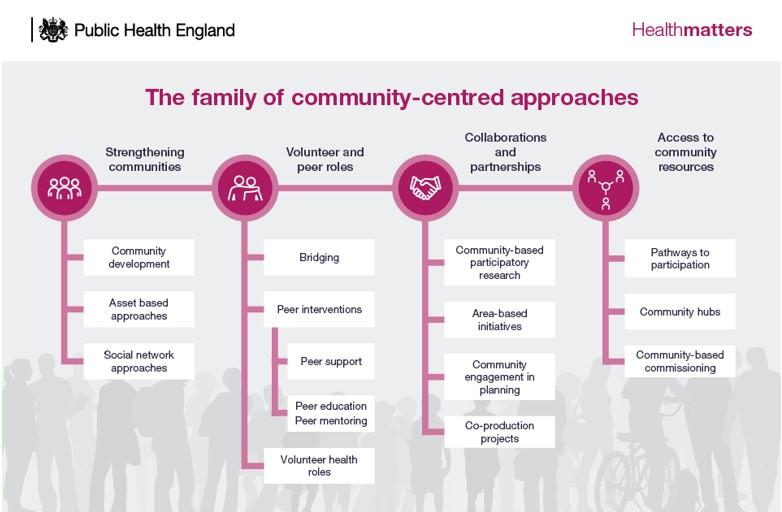
Source: Community-centred practice: applying All Our Health
We have identified a range of models in the case studies and literature review and these share some common characteristics including clarity about the underlying principles and key goals and building from existing infrastructure at the neighbourhood level. However, none of the models subscribe to a single methodology, but rather are flexible and borrow the principles from a range of sources that fit their context most effectively. Some of the approaches we have heard about include:
- Asset-Based Community Development (ABCD)
Building on community strengths and resources, ABCD involves identifying the assets a neighbourhood or community currently has and mobilising these assets to promote better health outcomes. - C2
A community empowerment model developed in the UK. It focuses on creating strong, sustainable partnerships between residents and local service providers to address complex social issues. - Local area coordination (LAC)
LAC is a ‘strengths-based’ approach that builds on what’s strong in people’s lives and communities. Local area coordinators are based in communities and are recruited together with the input of local people. They proactively meet with individual citizens and whole families in their neighbourhoods, building trust and connection with people over time. - Community hubs
Central points of access for co-located services and support. Hubs could be located in existing healthcare infrastructure or other locations such as schools or local business sites. - Whole-system approaches
An approach that uses systems thinking and tools to tackle complex problems with multiple drivers such as promoting healthy weight. It involves a very broad set of stakeholders working together to solve complex issues. - Personalised management model
Aimed at providing personalised care by assigning case managers to coordinate services for specific individuals. In the case management model, multiple services, both statutory and non-statutory, are co-ordinated by a given case manager to resolve issues for the individual they are working with. - Primary-care-led models
Multiple models exist that are led by primary care and many integrated neighbourhood teams are primarily led by primary care. The extent to which these are integrated with community services varies. - Social prescribing
Referral of residents to a range of local, non-clinical services that could be statutory- or community-led activity.
Glossary of terms
Community: A group of people who have a shared socially significant characteristic. The shared characteristic could be linked to where they live or based on other shared characteristics including faith, culture or interests. A neighbourhood is likely to contain several different communities who reflect the people living there and, similarly, a community may transcend several different neighbourhoods.
Integrated: Integration in health and care covers a range of activities from co-ordination between professionals around a specific set of individuals and needs, to a fully joined-up multi-disciplinary team with shared governance, funding, processes and systems, potentially aligned into a single organisational form. We have tried to distinguish in this report between integration based on bringing together people into a single set of processes, structures and form, and integration based on a focus on a shared set of integrated outcomes.
Neighbourhood: There is no single definition of neighbourhood, but there are often precedents based on geographic, historic, socio-economic, cultural and community factors. A neighbourhood is generally defined around a district or community and in the examples we have studied can extend in scale from a single row of residences to an area covering over 50,000 people.
Neighbourhood Working: in the context of this report, we focus on the way in which neighbourhoods – often self-defined and hyper-local – can provide the basis for communities and statutory services to work successfully together in improving health and wellbeing. This involves statutory and non-statutory partners aligning different assets, capabilities, capacities and experience to work towards a common improvement goal.
Place: Place in this context refers to the geographic level between system and neighbourhood, often shaped by local authority boundaries, where health and care partnerships are currently operating to develop better integrated health and care.
Statutory services: Statutory services are services that are required by law, are funded primarily through taxation, and are based on meeting the essential needs of the population, delivered by institutions including the NHS and local authorities.
System: System in this context refers to integrated care systems, the 42 statutory partnerships that cover the whole of England with a focus on prevention, better outcomes and reducing health inequalities through bringing health and care organisations within each of their footprints together to develop shared plans and deliver joined-up services.