
Towards integrated health organisations: considerations for policy and NHS leaders
Finding the right structure
How could partners come together?
Beyond a contractual relationship, providers across care pathways need some level of structural integration to facilitate collaborative planning and decision-making. Rather than a costly and disruptive reorganisation of the provider landscape, this should be approached in the spirit of evolution, strengthening the arrangements that already exist locally. As Browne Jacobson and the NHS Transformation Unit describe in their report, Collaborative Care, there are multiple approaches to provider collaboration available dependent on local circumstances. These range from statutory committees and joint ventures to lead provider or alliance models or shared leadership (but separate organisations), up to a single merged organisation (See figure 2).
Figure 2
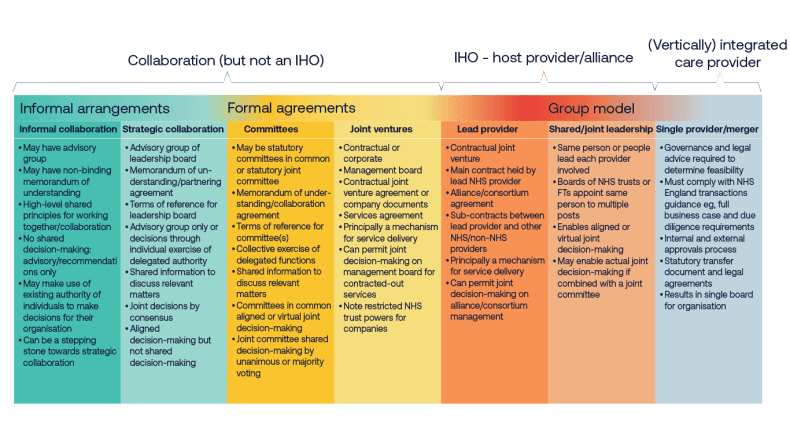
Figure 2. Levels of provider integration, taken from Browne Jacobson and the NHS Transformation Unit, Collaborative Care (2024).
This spectrum is not linear, and in a given area providers may choose to arrange themselves using a range of the approaches outlined in figure 2.
For an IHO contract, given that by definition a lead (better termed a ‘host’) provider sub-contracts partners, at a minimum a lead provider model is needed. This could be deepened with shared or joint leadership. Local partners should be empowered to choose the best model based on their local readiness and existing configurations. At its extreme, this could see all the providers become a single merged organisation. The merged organisation would provide all services in house without sub-contracting them. At this stage it will have evolved into an integrated care provider. Reaching this level of integration is not a realistic prospect in the near future for most areas, although it may happen sooner in areas with ‘neater’ provider arrangements where there are a smaller number of care providers and coterminous local authority boundaries.
Mental health providers are already using a collaborative model based on a lead provider to align incentives across multiple providers to de-invest in inpatient care and invest in community-based resources. The provider collaborative model in provision of specialist mental health, learning disability and autism services are established collaborative working arrangements, that have taken on specialised commissioning delegated budgets and functions from NHS England in recent years. Starting with commissioning a small number of specialist services in pilot sites, they have grown to cover all of England and the vast majority of specialist mental health and learning disability provision.
The collaboratives foster greater integration and better relationships between mental health providers, including independent and VCSE organisations where appropriate. In the East of England, the provider collaborative has significantly reduced out of area placements for children and young people. West Yorkshire Mental Health, Learning Disabilities and Autism Collaborative has reduced the number of people admitted to hospital, lowered spending on inpatient care and reinvested savings into community-based services. For further details and case studies see Annex 1.
Who can be the host provider?
A tension exists between who should host an IHO contract versus who could. The 10YHP stipulates only the ‘very best’ new FTs (as defined in annex 2 of the Advanced Foundation Trust guide) can become IHOs, limiting the opportunity to acute, mental health and community foundation trusts. Non-statutory NHS bodies, including primary care providers, are therefore not eligible under existing policy.
While NHS leaders have mixed views about which type of trust (acute, mental health, community, ambulance or mixed) may be best placed to take on the hosting role, there is consensus that the designated provider should be determined locally based on mutual agreement as to which provider is best placed to deliver its functions. The IHO host provider will also need different governance arrangements given its responsibility for population health, not just delivering activity and services.
The IHO will need to be led by someone and who that is will vary dependent on abilities and skills in different areas. It should be the organisation that is best placed, not because they are more dominant or involved but because they have the strength to get the alliance working.
There is a need to make sure it’s not an acute-led process and make sure everyone feels they have parity within the relationship. The relationship is not about the lead provider, it’s about equals coming together. The lead aspect is just a reflection of how the money flows.
A primary care lead provider could, in theory, offer the most coherent model for integrating physical and mental health services. For primary care to take on such a role, it would need to operate within a statutory framework that enables practices and primary care providers to come together as a corporate entity. Some trust leaders also expressed scepticism about the feasibility of IHOs being hosted by, for example, GP federations, citing concerns around their ability to manage risk and ensure organisational robustness. However, in areas which do have primary care at scale with robust formal governance, risk management and devolved decision-making, these bodies should not be ruled out of becoming IHO host providers in the longer term. GP federations are likely in many places to hold multi-neighbourhood contracts. This may provide them with the opportunity to stabilise the contracting, provide organisational robustness, and to explore NHS body status.
Regardless of who hosts the IHO contract, it will be essential that all parties to the IHO contract are fully engaged and incentivised to partner effectively within the arrangements.
The role of primary care
Leaders across all trusts and ICBs stressed the key role of primary care within the partnership arrangement; the breadth of primary care and not just general practice. Primary care leaders have a strong understanding of local population need, offer clinical leadership and will, in many cases, hold neighbourhood contracts. In the words of one community trust leader:
If you don’t establish an IHO in a way that includes primary care within the contract, you lose a huge lever to shift the balance of system finances.
In other models, such as ChenMed in the USA, GPs are employed directly by the equivalent IHO body, reflecting a vertically integrated approach to service delivery. However, the GP partnership model, comprising independent contractor businesses with self-employed GPs, is the main legal framework for delivering NHS general medical services in England. The same applies to many community pharmacies, optometry and dental practices who operate under the independent contractor model. This raises questions around the application of competition law, given that primary care providers, as independent contractors, are not formally constituted as NHS entities. Consideration should be given to whether this issue could be overcome by ensuring practices sit within an at-scale primary care provider, with alignment across SNP, MNP and IHO contracts.
Across England, general practice contracts have frequently been taken on by NHS trusts when practices have faced difficulties or risked closure. NHS trusts have rightly recognised the significant risk to the local health economy if these practices were to close and have intervened to ensure continuity of services. In some areas like Wolverhampton and Chesterfield, NHS trusts have taken on General Medical Services (GMS) contracts, thus directly employing GPs. But this approach is unlikely to become universal – at least not in the near future.
Many GP at-scale organisations have also successfully taken on GMS contracts for practices that have handed their contracts back and successfully managed these services within the GMS envelope. Going forward, these organisations must be empowered to support the stability of practices and, where required, support with the turnaround of practices.
Integrated models designed to support the delivery of GMS should include expertise in operating safely and efficiently within the GMS framework. This can be achieved through strategic collaboration with primary care at scale. Having a strategic partnership with an at-scale organisation could allow the continuity of services whilst returning practices to GP partners if viable and appropriate.
Including primary care provider leadership within IHO arrangements can be challenging due to the fragmented nature of primary care provision across and within general practice, community pharmacy, optometry and dentistry provision. But we are now seeing primary care provider collaboratives emerging across the country. These collaboratives are acting as both a voice and in many cases a provider of at-scale services.
The role of the ICB
In their new strategic commissioner role ICBs will increasingly be expected to commission care around the needs of populations, transitioning away from the existing activity-based model. IHO contracts will be one of the options available to do this. ICBs will be responsible for setting the parameters, outcomes and goals that IHO host providers are accountable to deliver on behalf of the population. ICBs will work closely with local partners including health and wellbeing boards and draw on their population health improvement plans to set these outcomes. They will use their expertise in population-level analysis, working closely with public health colleagues, patients and communities, to understand the priority areas for transformation. They will also be responsible for evaluating the impact of and delivery against that contract.
Currently, resource for primary care digital and analytics sits within ICBs, bar some pioneers like Birmingham and Solihull. However, agile, high-quality analytical capability at place level will be essential for transforming care from a predominantly reactive to a more proactive model. ICBs, alongside regional teams, will therefore need to support IHO host providers to develop this capability over time so it becomes the norm, not the exception.
ICBs will also help foster the conditions in which IHOs can thrive, giving providers the autonomy and operational independence to deliver IHO functions. This will require cultural change and a departure from their pre-10YHP role, which involved greater day-to-day operational oversight.
IHOs will likely see host providers assuming some ICB functions for their population, in line with the model ICB blueprint, which suggests functions will be delegated or contracted to providers over time. In many places this will take several years.
The most mature ICBs are already exploring how to hand over responsibilities to provider partnerships, recognising that strategic commissioning and operational delivery cannot be effectively managed at the same level.
Delegation of commissioning from ICBs is currently extremely limited. And ICBs’ timescales for delegating commissioning functions to providers will vary according to providers’ readiness to take on this responsibility – something which is impacted by current operational pressures.
Collaboration with local government
IHO host providers would be accountable for contracting healthcare services for their population. However, given their responsibility for improving population health, they will need to collaborate with ICBs and local government to do this. In the words of an acute leader:
It’s not an NHS only issue. A competent IHO needs to be leading collaborative working with local government.
IHO host providers could co-commission services with local authorities, as ICBs do, and IHO contracts could in future include service provision of Section 7A public health functions (following planned delegation of commissioning from regions to ICBs in 2027).
However, there are currently legal barriers to wider collaboration with local government. Mechanisms to pool budgets and delegate functions need strengthening. For example, something akin to Sections 65Z5 and 6 of the NHS Act 2006 for local government would provide an easier mechanism to delegate and share decision-making on health related and public health functions with other public authorities.
Additionally, the National Health Service Act 2006 stipulates that at least 51 per cent of a foundation trust’s income must come from the provision of NHS services. This threshold was originally intended to ensure that foundation trusts remain primarily focused on delivering NHS care. However, this requirement presents a challenge for IHO host providers, which may eventually seek to include services that span across public health and social care within their sub-contractual arrangements. This requirement should be changed to relate to public service income, not specifically NHS income.
Similarly, NHS Resolution’s indemnity schemes would need to be considered given that services may not be only provided by employed NHS staff. As IHOs may take on responsibility for social care and public health services, NHS Resolution’s indemnity remit may need to be broadened. Beyond legal limitations, joint working with local government is still limited and would require drastically improved relationships.
The role of the ‘integrator’
The relationship between the IHO host provider and ‘integrators’ will likely vary. In some areas the integrator and IHO host provider may be separate but complementary. In other areas whether the integrator is a lead provider, it may evolve into the IHO host provider if at an appropriate scale. Some healthcare leaders use the term ‘integrator’ to refer to an existing organisation operating as a host provider, supporting frontline teams by coordinating funding, data, workforce, estates, and other enablers. This role has been articulated in London’s target operating model for neighbourhood health. This integrator primarily hosts the necessary functions to enable neighbourhood working at scale, but in some areas also enables hospital-at-home and urgent community response services and coordinates integrated discharge. The integrator should provide the necessary infrastructure to enable a group of providers to work together in delivering neighbourhood health across multiple neighbourhoods through MNP contracts.