Embedding a more intelligence-driven and risk-based approach to the way NHS trusts and foundation trusts are regulated and monitored has been a welcome, key focus for CQC over the last 12 months.
CQC's new approach to inspections was introduced in 2017. In line with its five-year strategy, it involves moving towards a more responsive inspection model, in which resources are targeted to areas where concerns about quality of care are greatest. As part of this new approach, CQC made changes to the provider information request (PIR) to attempt to streamline the information that trusts are required to provide in advance of inspections.
Over the last 12 months, CQC has been carrying out the first round of well-led inspections, which were introduced as part of CQC's new approach to regulation and are based on the well-led assessment framework used by both CQC and NHS Improvement. Currently, trusts undergo a well-led inspection annually, approximately, following a targeted inspection of at least one core service. However, CQC has signalled that it intends to adopt a more risk-based approach to carrying out well-led inspection for trusts that are rated 'good' and 'outstanding' in future.
CQC and NHS Improvement also now report and rate use of resources (UoR) for non-specialist acute trusts. These assessments are carried out by a team from NHS Improvement who provide their findings to CQC in order for CQC to write the assessment report and decide a trust's UoR rating for use of resources. This rating is then combined with CQC’s existing five quality ratings for the trust.
This year has been one of continuity in terms of CQC’s approach to calculating fees for NHS trusts. CQC introduced changes to its fee structure in 2018/19 as part of its move to a full chargeable cost recovery model. As a result, CQC confirmed earlier this year that it will not make any changes to this methodology for 2019/20 - each trust will continue to be charged in proportion to its turnover levels and there is no minimum or maximum fee. This continuity is welcome, however there is a risk that CQC will be dependent on a small number of providers for a significant proportion of its income and CQC will need to recognise the impact of this on its relationships with those providers.
Care Quality Commission's new approach
As in previous surveys we asked respondents to reflect on their most recent CQC inspection and share their views on the process and their interaction with CQC. Last year we asked trusts for their early views on CQC's new approach which revealed that trusts were generally optimistic about the potential benefits it would bring. However, this year’s results suggest that trust leaders feel the benefits have not yet been felt at the frontline. This is explored in more detail throughout this chapter.
Four in five (80%) respondents to our survey said they had received a PIR within the last 12 months and 87% had received either a comprehensive inspection, core service with well-led inspection or focused inspection. Our findings therefore provide a valuable insight into how CQC's new approaches to regulating and monitoring providers are bedding in and the impact on trusts in practice.
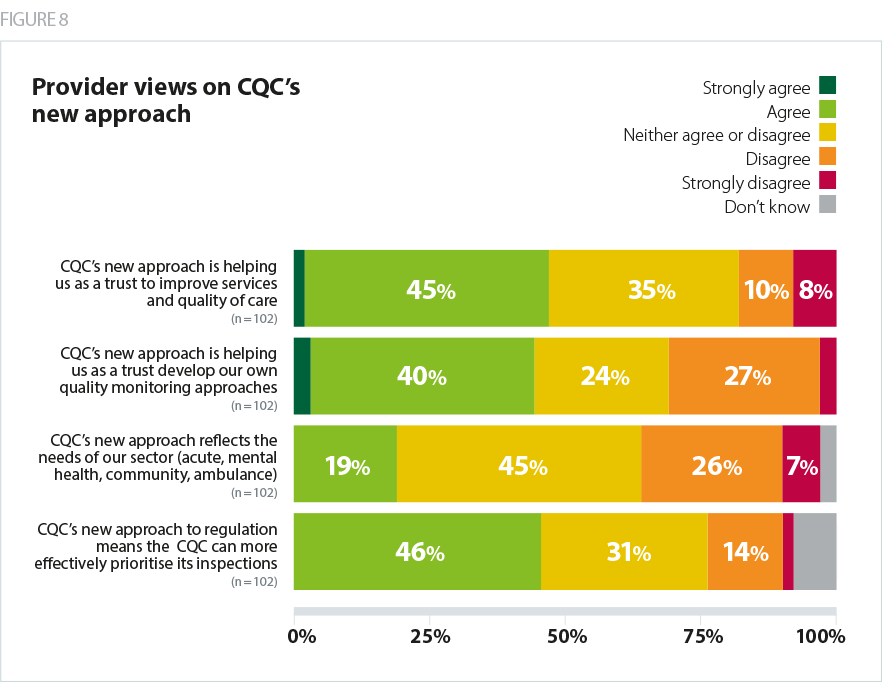
Just under half (47%) of trusts agreed that the new approach is helping them to improve services and quality of care. Last year, 63% of trusts said the new approach would help them to improve services and quality. Also just under half (47%) of trusts said they felt CQC's new approach is helping them to develop their own quality monitoring approaches. This is significantly below the proportion of trusts in last year's survey (80%) who expressed optimism that CQC's new approach was likely to help them to do so. Last year, 57% of trusts agreed that the new approach would provide a fuller understanding of quality of care, whereas this year, only 39% of trusts agreed that this was the case in practice.
Our findings around the extent to which the new approach reflects the needs of particular sectors also seems to suggest the experience of CQC's new approach over the last 12 months has fallen short of some expectations. This year, only 19% of respondents agreed that CQC's new approach reflects the needs of their sector, whereas 62% of respondents to our survey last year felt that the new approach was likely to have this effect.
The majority of respondents (81%) to last year's survey either 'fully' or 'partially agreed' that the new inspection approach was likely to enable CQC to prioritise inspections more effectively - this year only 46% of respondents said this was case in practice.
Taken together, the results suggest challenges remain as CQC moves to a more focused inspection model which includes annual well-led assessments. In our response to CQC’s consultation on the move to a new inspection approach, we highlighted the importance of training CQC inspection teams, ensuring the reliability of insights gained through the new intelligence model and importance of improving relationships with providers at the local level (NHS Providers, 2017). The feedback gathered in this year’s survey suggests trust leaders believe CQC could do more to equip, train and support inspection teams, as well as further refine its intelligence-driven approach.
Coordination with other national bodies
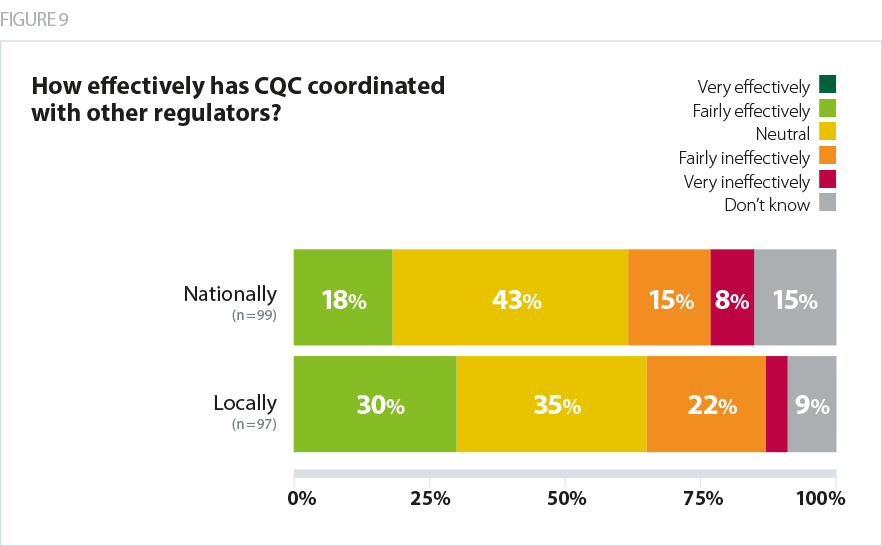
Trusts' opinion was divided as to whether CQC had coordinated its activity effectively with other regulators and national bodies locally (30% agree, 26% disagree, 35% neutral). On a national level, more trusts felt CQC had not coordinated effectively than those who did (18% agree, 23% disagree, 43% neutral). Trusts pointed out that there is more CQC could do to align its processes and requests with local bodies, as well as other national regulators. For example, one respondent highlighted that some ad hoc incident reporting required by CQC duplicates reporting to local commissioners.
There seems little or no co-ordination with other agencies to ensure that investigations can be done once and then not replicated.
[CQC PIR] is very burdensome. Much of the data is already provided to NHS Improvement so not clear why we are asked to provide it to CQC.
Benefits and challenges of inspection
As in previous years, we asked trusts to describe some of the benefits and challenges of inspection.
Only one in four (25%) trusts agreed the benefits of their most recent inspection justified the cost, which is a significant drop from last year (37%) and exactly half the proportion of trusts who felt the cost was justified when we first began surveying trusts on their views of the regulatory regime and its future in 2014.
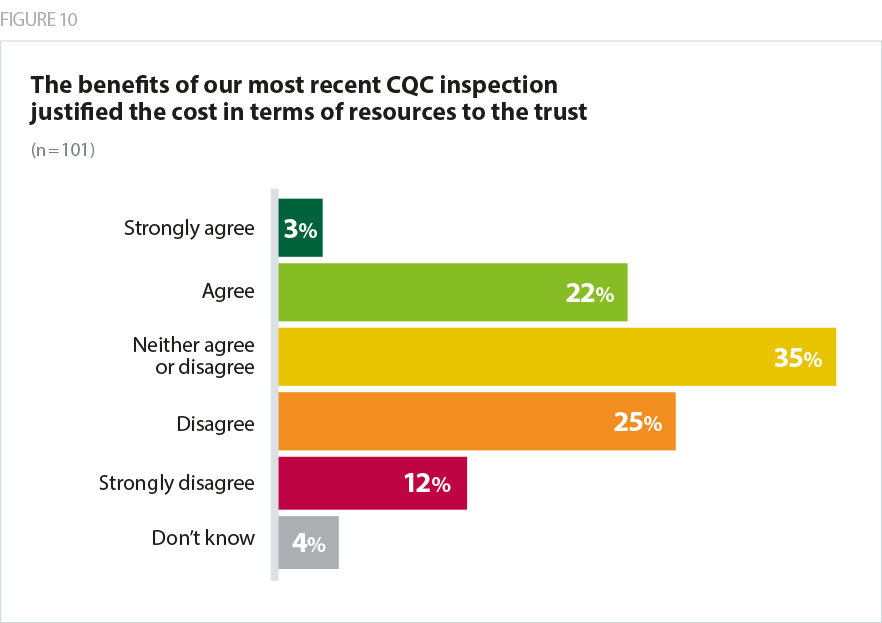
As was the case last year, respondents to this year’s survey highlighted that preparing for, and undergoing, CQC inspections divert significant attention and resources away from trust's main duties, and inspections offer less value for money as a consequence. While CQC fees were not explicitly referred to as often this year, these findings seem to suggest that the concerns raised last year about whether the benefits of CQC regulation and inspection justified the increase in fees in 2018/19 persist.
Also in line with last year's findings was the consistent message coming from trust leaders about the extent of administrative burden CQC's new approach places on their organisations. This year, 64% of respondents this year disagreed that CQC's new approach to regulation had reduced administrative burden, whilst only 11% of trusts agreed.
The amount of information requested - usually at short notice - is so large that it is disruptive to day to day functioning of the organisation during this period.
The PIR process was highlighted as particularly time consuming and burdensome, suggesting there are further opportunities to reduce the burden of data collection prior to, during and post-inspection. Trusts highlighted in particular challenges with the volume of data requested and the format the data needs to be submitted in, which does not match how some trusts collect data internally. Other trusts commented that the generic template means that not everything that would be relevant can be shared, or requests for information are made which are not relevant to particular sectors. Trusts also reported receiving duplicative requests - a number of trusts commented that they received requests for information that they had already provided through the PIR, or by other means, for example, to NHS Improvement. Finally, they also highlighted that requests are often accompanied by a short timeframe for submission.
I worry about the distraction from serving our patients quality care whilst trying to get data in a format that CQC wants - not necessarily what can be produced by our systems.
A number of trusts questioned the extent to which the PIR adds to CQC's overall assessment process, which is particularly concerning considering the amount of time and resource trusts are using to complete returns. A number of respondents said inspection teams had not appeared to have read their trust's PIR prior to the inspection, or the PIR data did not appear to have been taken into account in their trust's final CQC report.
It is… very frustrating when the data is provided to CQC and when the inspection team arrive they haven’t even read it and then ask for information that has already been provided.
The make-up of inspection teams continues to be a key area trusts identify for improvement. Respondents highlighted the importance of having experienced inspectors with the appropriate skills and knowledge, who are well-briefed on the trust and its context. As was the case last year, respondents also highlighted the importance of consistency, with several reporting that variation persists in the objectiveness of the judgements reached by inspection teams.
There is still too much variation in the quality of inspectors.
Some respondents did give positive feedback about the PIR process, commenting that it had been less burdensome than CQC’s previous approach. Preparation trusts took in advance and having completed a PIR before were highlighted as factors that made the process more manageable. This suggests that it may be possible for some of the issues trusts are experiencing to be overcome the more trusts get to grips with the new information collection process.
There were also a number of positive comments from trust leaders about the value of developing local CQC relationships and having more regular interaction with their local CQC teams.
Having a linked person at CQC has made a big difference to the trust especially when it comes to asking and getting answers to questions. A single point of contact has been very helpful.
The new CQC insight process has included regular interaction with core services in the Trust, which has helped in building relationships, and potentially means a better opportunity to present a balanced look at the core service.
I hope the new way of working with engagement throughout the year will reduce the burden.
It is a lot of work and paralyses an organisation for three months. A more data driven approach would be welcome.
Well-led
As with last year's survey, we asked trusts how useful the CQC well-led inspection had been for their organisation and to provide feedback on the assessment process.
Trusts have told us, separately to the survey, that the well-led framework and key lines of enquiry are useful and provide good structure for review, self-assessment and action planning. While trusts do think the local system they are working in or their contribution to the local system could be better reflected in CQC assessments and reports, their concerns tend to be with the CQC's approach to inspecting against the framework, rather than the framework itself.
This was borne out in comments from respondents to our survey. A number of trust leaders raised concerns about the experience and quality of well-led inspection teams, and suggested that this limited the value of the process and the feedback they received as a result. The importance of inspection team members having board experience as well as experience in the sector they are inspecting cannot be overstated.
Not a satisfactory experience due I suspect to the inexperience of CQC inspection team.
However, a number of respondents commented that their well-led inspection was a useful and constructive experience. In these cases, trusts felt they were given fair feedback and that the inspection provided a helpful, external perspective that focused their thinking or added to improvement work already underway in their organisations.
Well-led inspection is genuinely helpful process…that brought the board and executive team together and gave some insight into where we are as a trust. Fresh pair of eyes is always helpful.
Fair feedback with some good recommendations that the trust is taking forward.
In line with last year's findings, several respondents said there continues to be a lack of consistency between initial feedback they received immediately after the inspection and their final report. Several trusts also commented that the process continues to be resource and time intensive.
Overall, this year's survey results suggest there remains a general consensus that potential positive impacts of CQC's new approach are yet to be delivered in practice. Trusts recognise that CQC is in the initial stages of implementing its new approach and several respondents expressed hope that CQC will learn and refine it as time goes on. Our findings suggest more time for the new approaches to bed-in may help with some issues. However, more time alone will not remedy all of the issues trusts have raised, particularly the quality of inspection teams and the challenges system working presents to CQC's current sector-based model.
The approach to CQC inspection is still not risk based and has not reduced the burden of bureaucracy. We are hopeful that this may be addressed in 19/20.
I do believe that CQC are interested and listening and I am hopeful that the process will improve in the future.
CQC local system reviews
The environment within which trusts are operating is changing fundamentally. It is important that the regulatory framework is flexible enough to take account of these changes and does not prevent the provider sector from innovating and working in new ways to deliver new integrated models of care and system collaboration.
CQC has set out broad principles underpinning how it is seeking to adapt its regulatory approach to take account of the evolving ways in which care is being delivered, both in terms of the move to system working, and in relation to 'complex' providers – trusts delivering a range of services that cross traditional sector boundaries, such as acute care and mental health care, and increasingly, primary care and social care. CQC has put forward welcome proposals for monitoring and inspecting complex providers, including putting in place a single CQC relationship-holder for each provider.
CQC's existing sector-based model was raised by respondents as a concern, with some trust leaders commenting that CQC inspections struggle to assess integrated care pathways or services that span sectors. 28% of trusts said CQC's approach to regulation is a barrier to delivering integrated care, while 34% disagreed.
CQC has also reflected the move to system working in its approach to regulation. CQC completed its programme of local system reviews of health and social care in 23 local authority areas and published the report Beyond barriers in July 2018 (Care Quality Commission, 2018). The local system reviews, carried out under special powers at the request the secretaries of state for health and social care and housing, communities and local government, focused on care for older people across a whole system. CQC found that, while there are often good intentions to work together and good planning between services, organisations mostly focus on their own goals and are not funded in a way that supports them to work together.
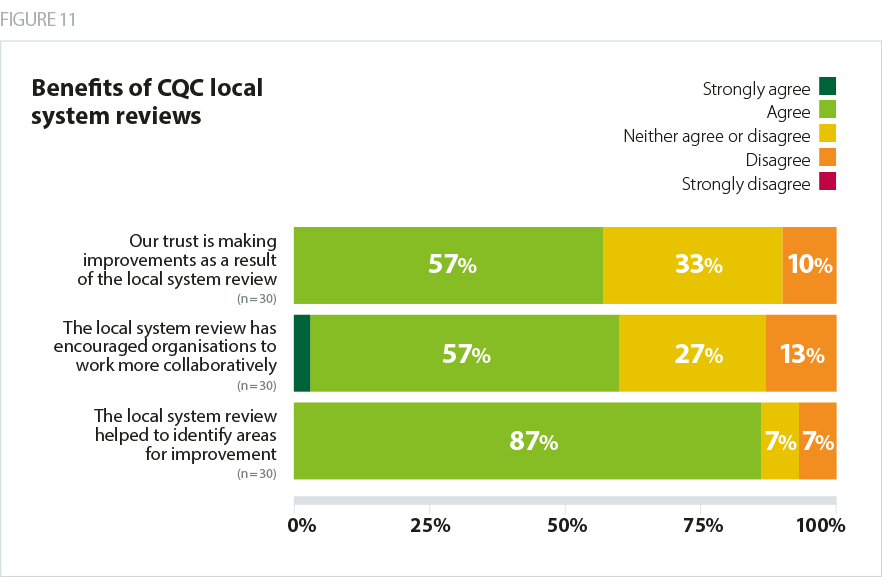
Just under a third (30%) of trusts that responded to our survey had been involved in a CQC local system review. As shown in figure 11, the overwhelming majority of these trusts (87%) agreed the local system review had helped identify areas for improvement. A majority of them (60%) also agreed the local system review had encouraged organisations in their system to work more collaboratively, and over half (57%) said they are making improvements as a result of their local system review.
Given these findings, it is welcome that the Department for Health and Social Care has confirmed it will commission CQC to carry out further local system reviews. CQC is currently considering the focus of these reviews.
There is much that the national bodies can learn from this programme as they progress the development of new models of oversight at system level. Some trusts had already commented, separately to this year’s survey, that the reviews had been well received given their welcome focus on improvement, as opposed to performance management or pleasing the regulator, because CQC cannot take regulatory action against systems (NHS Providers, 2019).
I believe that the greatest challenge to regulation will be the way in which CQC is able to assess, but more importantly reflect and describe what organisations are achieving and delivering at a system level.
As CQC makes further progress on adapting its approach in response to the changing operational context for providers in particular, CQC must work with other national bodies to ensure their approaches are aligned. A crucial element CQC needs to consider is how, when designing system-level assessments, it will work with NHS England and NHS Improvement to ensure that its approach is aligned with ratings for STPs/ICSs, in order to ensure providers and their system partners will not be subject to multiple judgments. The chapter of this report on oversight and regulation of systems and new organisational forms considers these issues in further detail.
Acute inspections are designed around single site acute hospitals and are not well adapted to assess integrated care pathways or 'group' organisations.
[CQC] needs to shift… to systems not organisations.
Use of Resources
Close to half of all trusts (47%) told us they have had a Use of Resources (UoR) assessment in the last 12 months. There was a fairly even number of positive and negative comments about how helpful the assessment had been and the assessment process itself.
Some respondents felt that the assessment process offers a valuable opportunity for self-reflection. However, a number said the external assessment did not add value beyond what the trust already knew. Others felt it was still valuable to have an external perspective validate the trust's own assessment.
A number of respondents highlighted the resource-intensive nature of the assessment, with a few describing it as unstructured. There were concerns about members of the review teams lacking senior experience and some reports that feedback provided on the day was subsequently contradicted in the final report and rating.
Other comments concerned the data used to guide assessments, with trust leaders suggesting that data is not always up to date, or that it fails to adequately reflect their trust, for example where they are delivering integrated services that span traditional sector boundaries. As in previous years, leaders of non-acute trusts told us that they would like the UoR framework and assessments to be widened to include their sectors.
A number of trust leaders also reflected the view that UoR is a blunt tool and not nuanced enough to properly reflect an organisation’s position, in particular, the reasons why a trust may be in deficit. There was a sense among some respondents that their UoR ratings were automatically limited by their organisation’s underlying cash position and/or performance against control totals - therefore it was unclear what value the UoR assessment itself added.